Epistemology and the Feldenkrais Method
Abstract:
Research takes place within a paradigm, which rests, in turn, on an epistemology, or theory of knowledge. Good research paradigms for the Feldenkrais Method do not exist, in part because conventional scientific epistemology does not adequately represent forms of knowledge important to the Method. This article discusses this inadequacy and explores one possible approach to developing a non-conventional epistemology to address it.Introduction
In The Structure of Scientific Revolutioni, Thomas Kuhn describes science as a process organized around paradigms which he defines as consensual frameworks for deciding what questions are legitimate and what means are legitimate for answering those questions, agreed on by the community of researchers within which the research occurs. Most research takes place as part of what he calls normal science, guided by well established paradigms that define and provide a framework for exploring the questions that the discipline involved finds relevant. Examples of paradigms would include Newtonian mechanics, Copernican astronomy, wave optics, and organic chemistry.
In any field there are anomalies questions that the existing paradigm is unable to answer and data that it is unable to explain. As long as there are not too many anomalies, they can be pushed off to the side and ignored, and the process of normal science can go on unimpeded. Eventually, though, the anomalies build up to the point that they can no longer be ignored. The existing paradigm breaks down, and after a somewhat chaotic period of transition, the discipline adopts a new dominant paradigm. Kuhn calls this period of transition scientific revolution. The transition from Newtonian to relativistic mechanics would be an example. He notes that process by which a new paradigm emerges can be as much a political process as a scientific one, where personalities and persuasive abilities play more of a role than do purely scientific considerations.
In the Feldenkrais community, we don’t yet have good paradigms within which to do normal science. One way around this dilemma is to work within existing paradigms from other fields, such as medical research paradigms for assessing the effectiveness of drug therapies or other treatment interventionsii. There is some value in research that fits the Feldenkrais Method into such conventional research paradigms, particularly when it comes to marketing and to gaining legitimacy with the medical community. But such research often requires treating the Method as a simpler and more routinized process than it really is. Statistical assessments of the effects of the Method for some specific medical condition, in particular, are likely to view any Awareness Through Movement (ATM) or Functional Integration (FI) used in the research as routinized procedures following fixed protocols that can be replicated with other subjects to produce the same effects on the targeted condition. Such research may certainly be used to argue that the Feldenkrais Method is effective in whatever situations that effectiveness was demonstrated, but it is unclear that it will provide information of value to the continued development of the Method. Carl Ginsburg has written about some of the issues involvediii.
If we really want research that can significantly add to our deeper understanding of what we do and how we do it, we need to develop paradigms to guide that research that capture the richness and complexity of the Method. This, in turn, may require even more fundamental thinking about the epistemology — the theory of knowledge, the deeper agreement on the nature of knowledge and the means for determining its validity — upon which those paradigms rest. Our work is best understood through ways of knowing and validating knowledge not recognized by the conventional epistemology that underlies contemporary science, so we may need to develop our own broader epistemology as well.
The nature of conventional scientific epistemology
Conventional scientific epistemology requires knowledge to be objective, codified, unambiguous, and reproducible, in the following senses:
- Objective means that the knowledge adheres to the world “out there.” It describes objective characteristics of the phenomenon being described, independent of who is observing that phenomenon.
- Codified means that the knowledge is completely encoded in external symbolic (verbal or mathematical) form, separate from the knower. If you understand the words, you should understand the knowledge. Conversely, if you can’t put what you know into words such that other people can understand and reproduce it from those words, it isn’t knowledge.
- Unambiguous means that there is one right answer. Given two competing explanations for the same phenomenon, only one can be right.
- Reproducible means the phenomenon being described will look the same to every observer, and each time it is looked at.
I’ll refer to knowledge that meets these criteria as conventional knowledge — that is, knowledge that has been encoded in language or other symbolic form and can be duplicated by others. Scientific epistemology does not value non-verbal ways of knowing or non-verbal knowledge that may be difficult to transmit unambiguously from one person to another.
Individual scientists often step outside these boundaries in discovering and creating new knowledge. Subjective non-verbal understanding and intuition can be invaluable parts of the individual creative process, but the collective process discounts and obscures this. Well known examples include Einstein’s image of riding on a light beam and Kekule's dream of a snake swallowing its tail, which led to the understanding of the chemical structure of the benzene ring. But these intuitive discoveries became acceptable knowledge only after they were codified and logically validated.
One of the most important personal lessons I learned in graduate school, from the world-class mathematician who was my mentor, was to approach mathematical research as an intuitive rather than a logical activity. New mathematical knowledge flows from the mathematician's intuitive gestalt for the abstract structure he works with. The codified logical form that knowledge eventually takes on comes later — a means of recording and transmitting the knowledge, but not of discovering it. The formal system does its best to obscure the underlying process on which it depends for its existence.
Knowledge in a Feldenkrais context
Much of the knowledge on which the Feldenkrais Method depends is conventional knowledge. It can be and is codified within conventional epistemology. This includes, for example, knowledge about anatomy, neurology, some understanding of functional connection, etc. But there is also much that can’t be so codified — much which is non-verbal and perhaps ultimately impossible to put into words. As practitioners we depend on our ability to sense, connect, and communicate at deep intuitive levels. I’ll refer to these ways of knowing as non-conventional knowing or non-conventional knowledge. Different practitioners use non-conventional knowing in different ways and to different degrees; no single way of doing it is “right.” Different practitioners have different images of what we do and how we do it. We don’t all share the same descriptions of our knowledge, even when we share a deeper gestalt for what we know.
Non-conventional knowing does not fit within conventional scientific epistemology. It could even be argued, in fact, that this epistemology evolved specifically to reject and exclude non-conventional knowing, because it was seen as tantamount to mysticism and superstition. Scientists who draw on non-conventional knowing as a source of insight must translate what they discover into conventional codified form in order to get their work recognized; they must move beyond and obscure the non-conventional source. As Feldenkrais practitioners, we don’t have the option of obscuring our non-conventional sources and pretending that our work is independent of them. We must stay in touch with these realms, using intuitive information and communications throughout our work.
Elements of non-conventional knowing
Conventional scientific epistemology requires that knowledge be objective, codified, unambiguous, and reproducible. Let’s look at how the non-conventional knowledge important to a Feldenkrais practitioner might fail to meet those criteria, and why we might need a non-conventional epistemology to encompass them. Let’s consider the process a physician might go through in diagnosing and treating a patient and compare it with how a Feldenkrais practitioner might interact with a Functional Integration student.
The physician works within a paradigm organized around the diagnosis and treatment of pathology. He begins by identifying and collecting measurable objective data about the patient. When enough data has been collected the physician makes a diagnosis — identifying the patient as belonging to the class of people who exhibit a particular pathology. The data that the physician uses to reach his diagnosis are conventional facts, described by objective, codified diagnostic criteria. The diagnosis is also an objective, codified description identifying the diagnostic category to which the patient is assigned. Diagnosis is followed by treatment, which consists of applying an objective, codified protocol that has been accepted as appropriate for that diagnosis.
Throughout this process, the physician is applying and is guided by conventional knowledge — objective, codified facts that should look the same to any trained observer, and lead to the same unambiguous conclusions (diagnosis) and actions (treatment), no matter who does them. Faced with the same patient, in other words, competent physicians should come to the same diagnosis and apply the same treatment. It may not always work out that way in practice, but that’s what the system sees as the ideal.
Now consider a Feldenkrais practitioner engaged in a Functional Integration session. She also makes an assessment of her student’s situation, but in a far more subjective manner than the physician. She is looking less for specific indicators of specific conditions than for things that may appear out of balance somehow. She may look for a particular set of indicators, or she may simply respond to “what pops up.” She takes in information through a variety of sources and uses that information to guide her interactions with her client. Some of what she responds to may be readily describable in conventional terms — “his breathing was restricted,” for example, or “he couldn’t properly bear weight on his right leg.” But she may also sense larger and more diffuse patterns of connection or activity that have no conventional description, responding to them and integrating them into her interaction to the client without ever verbalizing them, even to herself, or bringing them fully to consciousness.
There are no standards of treatment for the Feldenkrais Method, tying specific diagnoses to specific treatment protocols, as there are in medicine. Different practitioners might approach the same student very differently. Some might address the student’s presenting problem very directly, some less directly, and some not at all — preferring to work with the student more globally and see what emerges. This individualized approach and lack of reproducibility is an important aspect of the Method.
A two-phase process of first collecting information and then deciding what to do about it, akin to but somewhat looser than medical diagnosis and treatment, may sometimes be present in Functional Integration, or it may be completely absent. Sometimes the practitioner only collects information — continually asking, in effect, “What’s happening here now?” but without acting on the answer, as a physician might. Instead, she simply notices and moves on. Bringing information to awareness produces change, so the next time she comes back to the same place to ask the same question, the answer will be different. The practitioner’s skill in this process lies not in action she takes as a result of what she finds, but in her ability to select a trajectory along which to move while asking ”What’s happening here now?” that will produce beneficial change for the client.
The reproducibility and lack of ambiguity so important to conventional knowledge are not present here. The same practitioner, asking the same somatic question, may find a different answer every time she asks. Different practitioners will not only find different answers to the same question, they are likely not even to ask the same question, or even to be in agreement about what kinds of questions to explore. And yet all may produce good results, and the results may have more in common than the different approaches which produce them.
The beginnings of a non-conventional epistemology
So what might a non-conventional epistemology that would allow some of these non-conventional ways of knowing to be taken into account look like? How would it differ from the conventional epistemology used in contemporary science? I don’t have complete answers to those questions, but research that I did in the 1970s concerning the application of subjective judgment in combination with formal analysis to “squishy” public policy and planning problems suggests one way of conceptualizing the issueiv.
Think about the problem of a human actor faced with some substantive situation in the real world that he needs to address, and the relationships between the actor, the situation, and whatever models of the issue he uses in his decisionmaking. (I’m using the word model here to include all kinds of representations — physical or mathematical models, verbal descriptions, visual or other imagery, etc. — which the actor might use to encapsulate his knowledge and understanding of the situation.)
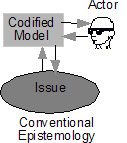 Conventional epistemology, in effect, restricts the actor to a single codified model — the externally agreed-upon “truth” describing the situation. It tells him to equate the situation with that model in his decisionmaking process. He should substitute the model for the actual situation and act in the manner specified by the model. He is, in effect, treating the model as a surrogate for the situation, within the meaning discussed below. And since there is a single agreed-upon truth that describes the situation, any other actor should understand the situation in the same way and choose the same action.
Conventional epistemology, in effect, restricts the actor to a single codified model — the externally agreed-upon “truth” describing the situation. It tells him to equate the situation with that model in his decisionmaking process. He should substitute the model for the actual situation and act in the manner specified by the model. He is, in effect, treating the model as a surrogate for the situation, within the meaning discussed below. And since there is a single agreed-upon truth that describes the situation, any other actor should understand the situation in the same way and choose the same action.
In the medical diagnosis and treatment paradigm discussed earlier, the codified model would include diagnostic criteria and approved treatment protocols for relevant medical pathologies. The physician’s job can be seen as one of matching diagnostic criteria with the patient's symptoms to reach a diagnosis, then applying a relevant treatment protocol. There may be additional complications in practice, but in principle, this is what’s involved.
Non-conventional epistemology, on the other hand, must allow the possibility that the actor may understand or describe the situation in more 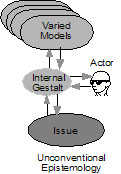 than one way. These might include codified models like those used by conventional epistemology, visual or kinesthetic imagery, gut feelings and other intuitive feelings, and other non-conventional forms. These are shown as a stack of varied models in the figure. None will necessarily be surrogates in the sense that the single model does in conventional epistemology. Rather, they may all serve as perspectives, feeding and enriching the internal gestalt through which the actor interacts with them and ultimately makes decisions about the situation. Different actors may use different models and different internal gestalts, leading to different ways of acting in the same situation.
than one way. These might include codified models like those used by conventional epistemology, visual or kinesthetic imagery, gut feelings and other intuitive feelings, and other non-conventional forms. These are shown as a stack of varied models in the figure. None will necessarily be surrogates in the sense that the single model does in conventional epistemology. Rather, they may all serve as perspectives, feeding and enriching the internal gestalt through which the actor interacts with them and ultimately makes decisions about the situation. Different actors may use different models and different internal gestalts, leading to different ways of acting in the same situation.
 To better understand the distinction I’m making here between a model as a perspective rather than a surrogate, think about two-dimensional images of three-dimensional objects, such as the picture of the cars shown here. The object being represented — the car in this case — has a greater dimensionality than the representation being made of it, the two dimensional picture. It’s not possible to create a two-dimensional image that unambiguously captures the object, because two dimension images simply aren’t rich enough to serve as three dimensional surrogates.
To better understand the distinction I’m making here between a model as a perspective rather than a surrogate, think about two-dimensional images of three-dimensional objects, such as the picture of the cars shown here. The object being represented — the car in this case — has a greater dimensionality than the representation being made of it, the two dimensional picture. It’s not possible to create a two-dimensional image that unambiguously captures the object, because two dimension images simply aren’t rich enough to serve as three dimensional surrogates.
Yet two dimensional representations can still provide very useful models of three dimensional objects. This is because we know there’s more to the object than what the picture shows. We use the picture to inform and enhance a richer internal understanding of the object being depicted. This internal understanding is what I referred to above as the actor’s internal gestalt. We can use a number of different views, from different perspectives, to give us a richer gestalt than we could obtain from any one viewv. That internal gestalt can be further enriched by additional models of other kinds — audio recording of engine noise, descriptions of performance and the driving experience, for example, for the car depicted here.
Objective codified descriptions of the kind required by conventional epistemology are no more capable of fully describing the rich and complex interactions that occur between Feldenkrais practitioners and our clients than two dimensional images are capable of fully capturing three dimensional objects, though they may usefully serve as perspectives on those interactions. A non-conventional epistemology along the lines described above might offer a useful way thinking about and modeling those interactions, and a base upon which paradigms for describing the Feldenkrais Method might be developed. I haven’t fully articulated such an epistemology here, certainly. But I hope this article at least illuminates the possibilities and suggests directions for further research.
iKuhn, Thomas. The Structure of Scientific Revolution. Chicago: University of Chicago Press, 1962. I recapitulate Kuhn’s main arguments in my chapter on “Science as a perceptual process” in The Reality Illusion: How you make the world you experience. Los Angeles: Somatic Options, 2000. <http://www.somatic.com/real_illus.html>
iiStephens, Jim, “Evaluating Research on the Feldenkrais Method from the Outside. Some Observations and Suggestions,” IFF Academy Feldenkrais Research Journal 2004 Vol 1, <http://iffresearchjournal.org/volume/1/stephens>
iiiGinsburg, Carl, “Reply to Jim Stephen’s First Version of this Article From 1999,” IFF Academy Feldenkrais Research Journal 2004 Vol 1. <http://iffresearchjournal.org/volume/1/ginsburg>
ivTwo examples of this research can be found on my website at <http://www.somatic.com/articles.html#rand>:
Strauch, Ralph. Risk Assessment as a Subjective Process, The Rand Corporation, Santa Monica, CA P-6460, March 1980, and Strauch, Ralph. ‘Squishy’ Problems and Quantitative Methods. Policy Sciences Vol. 6 (1975): 175-184.
vSome of these ideas are also discussed in more depth in The Reality Illusion, op. cit.
(2007). Epistemology and the Feldenkrais Method.
Feldenkrais Research Journal. 3, 6.
| Attachment | Size |
|---|---|
| 7-Strauch__IFF_Vol3_2007.pdf | 99.48 KB |