Awareness Through Movement Sequence on Fibromyalgia Patients
Abstract:
The purpose of this study was to describe the effects of a Feldenkrais Awareness Through Movement (ATM) sequence on fibromyalgia patients. Subjects met twice a week for a one hour group ATM lesson, and were instructed to follow through daily with practice tapes: After two months, subjects were placed on a one month home program. Pre-test and post-test data, which included a modified Fibromyalgia Impact Assessment (FIA) questionnaire, a pain scale, photographical postural analysis, and observational video analysis of walking, were collected and analyzed on five fibromyalgia patients. A paired t-Test on the modified FIA and other descriptive analyses showed moderate improvement in the subjects. It was concluded that the Feldenkrais Method has potential value as a possible adjunct to the physical therapy treatment of selected fibromyalgia patients.Julie R. Dean, Suzanne A. Yuen and Stacy A. Barrows, PT,CFP
Stacy Barrows can be reached at E-mail sabccpt [at] aol [dot] com or www.centurycitypt.com
Introduction
Fibromyalgia or fibrositis is the most common cause of severe musculoskeletal pain in persons seen by physicians, especially rheumatologists. (1) Although persons with fibromyalgia display diffuse musculoskeletal pain, chronic fatigue, sleep disturbance, and tender point sensitivity (1,2,3), medical tests show no significant abnormalities. Secondary symptoms associated with this disorder may include morning stiffness, headaches, gastrointestinal problems, depression, soft tissue swelling, paresthesia, menstrual changes, temporomandibular joint dysfunction, vertigo and thyroid problems. (2,4) Also, certain etiological factors such as emotional distress, trauma, noise, repetitive motion and climate, especially heat and lights, have been reported to exacerbate symptoms. (2,4) Poor postural habits have also been shown to aggravate fibromyalgia symptoms. (2,4)
Treatment programs for individuals with fibromyalgia have been diverse and varied, and as yet no one single treatment has worked for every patient. Some patients have reported partial symptom relief with tricyclic drugs (7), while others have experienced success with traditional modalities such as heat and ice. (1) Treatment through active stretching, postural education, body mechanics, and other forms of therapy has also provided some benefits. (1,2) Specifically, it has become apparent that persons with fibromyalgia benefit from aerobic conditioning and other exercise programs. (8,9,10,11,12) According to standards for fitness developed by the American Heart Association for a normal population, showed that 80% of patients with fibromyalgia are physically unfit. (13) McCain and colleagues conducted two studies involving aerobic exercise with fibromyalgia patients. (11,12) One study showed that pain scores, pain diagrams, and total myalgic scores improved significantly after a program of cardiovascular exercise. (12) The other showed only modest improvement in pain and other fibromyalgia symptoms measured. (11) Bennett hypothesized that a decreased activity level in fibromyalgia patients, and therefore decreased level of fitness, was due to patients' chronic pain and fatigue, making them more susceptible to muscle microtrauma: (8) Nichols and Glenn hypothesized that a program of aerobic exercise might increase the resistance of muscle to this microtrauma. (14) Results from this study were inconclusive. In fact, patients actually rated the disability section of their assessment as being higher after the program. Results vary among the few studies looking at exercise with fibromyalgia. One problem causing these varied results could be poor compliance to exercise programs. This decreased compliance may be the result of pain, fatigue, and a lack of personal efficacy. (8,10,13)
Physical therapy has been called upon to assist the patient to a more comfortable means to exercise and assume ease of posture and functional activities. There have been multiple philosophies of therapeutic exercise and neuromuscular reeducation used in the past. Recently, physical therapists have become aware of another approach called the Feldenkrais method. By clinician report, this approach has assisted patients with diagnoses such as cerebral palsy, stroke, and head injury. The approach is designed to assist individuals in reorganizing their movement patterns kinesthetically. (15,16) While there is limited research on this, proper application of this method may lead to reduction of pain, stress, muscular tension and soreness, and may increase flexibility and efficiency of movement. (15,17,18,19) Brown and Kegerreis showed that normal subjects perceived movements easier to perform after Feldenkrais sessions, thus furttier supporting the claim that the Feldenkrais method facilitates movement by helping the person reorganize the biomechanics of the movement, therefore decreasing effort used and increasing efficiency of the movement. (20)
The Feldenkrais method is divided into two modes of instruction: 1) Awareness Through Movement (ATM), and 2) Functional Integration (FI). In ATM, individuals perform small, gentle movement patterns, usually in a group setting, in response to verbal or written cues. The movements are self-directed and performed within each person's comfort range. Mental imagery of the movements is encouraged if the movements are perceived by the patient or the instructor to be too difficult. Mental imagery is also occasionally used as part of the lesson for all participants. Mental imagery has been widely studied and documented for its positive effects on learning. (21,22) The literature supports the view that mental imagery has also been found to enhance awareness-of the body. (22) In contrast, FI is individualized instruction. The individual is guided hands-on by a Feldenkrais practitioner, who may be a physical therapist, through gentle and slow movements. (15,18,23)
The Feldenkrais method functions to increase the person's sensitivity and awareness of physical movement. (18) Its aim is to improve the individual's ability to learn by reprogramming the sensorimotor learning ability of the central nervous system. (23,24) This ability of the central nervous system to learn and relearn movement patterns and its controlling influence over other components of movement has long been recognized. (5) The Feldenkrais method encourages "practitioners to work with patients in an instructional manner, rather than attempting to correct them." (24) By experimenting with movement, the central nervous system begins to distinguish which body positions are more or less efficient and thus helps to improve the person's gross motor ability. (23,24) This process is much like the experimental and explorative movement that helps a baby progress through the developmental motor milestones. (16,23,25)
The effectiveness of the Feldenkrais method has been documented in only a few studies. Case studies demonstrated that the method has reduced pain in patients with acute and chronic back problems. (15) A study by Ruth and Kegerreis reported increases in neck flexion range of motion after participating in a Feldenkrais ATM sequence. (26) Because of the lack of clinical studies on the Feldenkrais method, more research is needed to substantiate its validity as an appropriate treatment philosophy.
Instead of depending on short-term passive therapy to temporarily relieve their symptoms, fibromyalgia patients should be encouraged to take the initiative to progress towards long-term management. Long-term management involves assisting the patient to be responsible and self-reliant in participating in an active exercise program. (1,3) In order to enhance the ability of the patient with fibromyalgia to exercise and to move within an dynamically efficient postural alignment, the Feldenkrais method was evaluated for its potential use in reducing pain and improving kinesthetic sense. Decreased pain and improved kinesthetic sense would provide the patient with more comfortable movement choices to increase the capacity for physical movement.
The purpose of this study was to describe the effects of a Feldenkrais Awareness Through Movement sequence on fibromyalgia patients using a modified Fibromyalgia Impact Assessment, pain scale, photographical postural analysis, and observational video analysis of gait.
Methods
Subjects:
Initially, nine fibromyalgia patients, who self-reported as being diagnosed with fibromyalgia, were recruited by rheumatologist referral and from several Southern California Fibromyalgia support groups. No documented physician confirmation of the diagnosis was obtained. All subjects were female, whose ages ranged from thirty to fifty-one years-old, and dates of fibromyalgia diagnoses ranged from 1986 to 1994 (Table 1). Exclusion criteria included any person(s) involved in litigation, and any individual(s) with a medical condition that would prevent consistent participation in the study. A sample of convenience was used to provide for an experimental group only, with no attempt at random selection. Before participation, all subjects signed informed consent forms approved by the Mount St. Mary's College Human Subjects Committee. After one week, one subject voluntarily discontinued her participation in the study. During the course of the study, three subjects experienced acute onset of medical conditions. Data from these individuals were excluded from group analysis; however, for individual case study, data from one of the excluded subjects (i.e. Subject 6) was retained and analyzed descriptively . Pre-test and post-test data, therefore, were collected and analyzed on the remaining five fibromyalgia subjects.
Table 1: General Subject Characteristics
| SUBJECT # | AGE (YEARS) | ONSET OF FM SYMPTOMS (DATE) | DATE OF DIAGNOSIS | OTHER TREATMENT INTERVENTIONS | OTHER MEDICAL PROBLEMS |
|---|---|---|---|---|---|
| 1 | 47 | 1992 | 1994 | PT | OA, LBP |
| 2 | 33 | 1989 | 1989 | acupuncture, massage | LBP, CFS, HoTN2 to CFS |
| 3 | 49 | 1993 | 1994 | PT, OT, BFB, chiropractor, massage | LBP, tendonitis, bursitis, mental illness, ulcer or other stomach disease, depression, anxiety |
| 4 | 51 | 1984 | 1987 | PT(massage), trigger point injections, pain management program | LBP, ulcer or other stomach disease, anemia or other blood disease, depression, anxiety, allergy and sinusitis |
| 5 | 37 | 1990-1994 | 1994 | PT, BFB, chiropractor | OA (neck), tendonitis, carpal tunnel syndrome?, ulcer or other stomach disease, depression |
| 6* | 30 | 1993 | 1994 | LBP, tendonitis/bursitis, anemia or other blood disease, depression, anxiety, amenorrhea, CFS |
PROCEDURE:
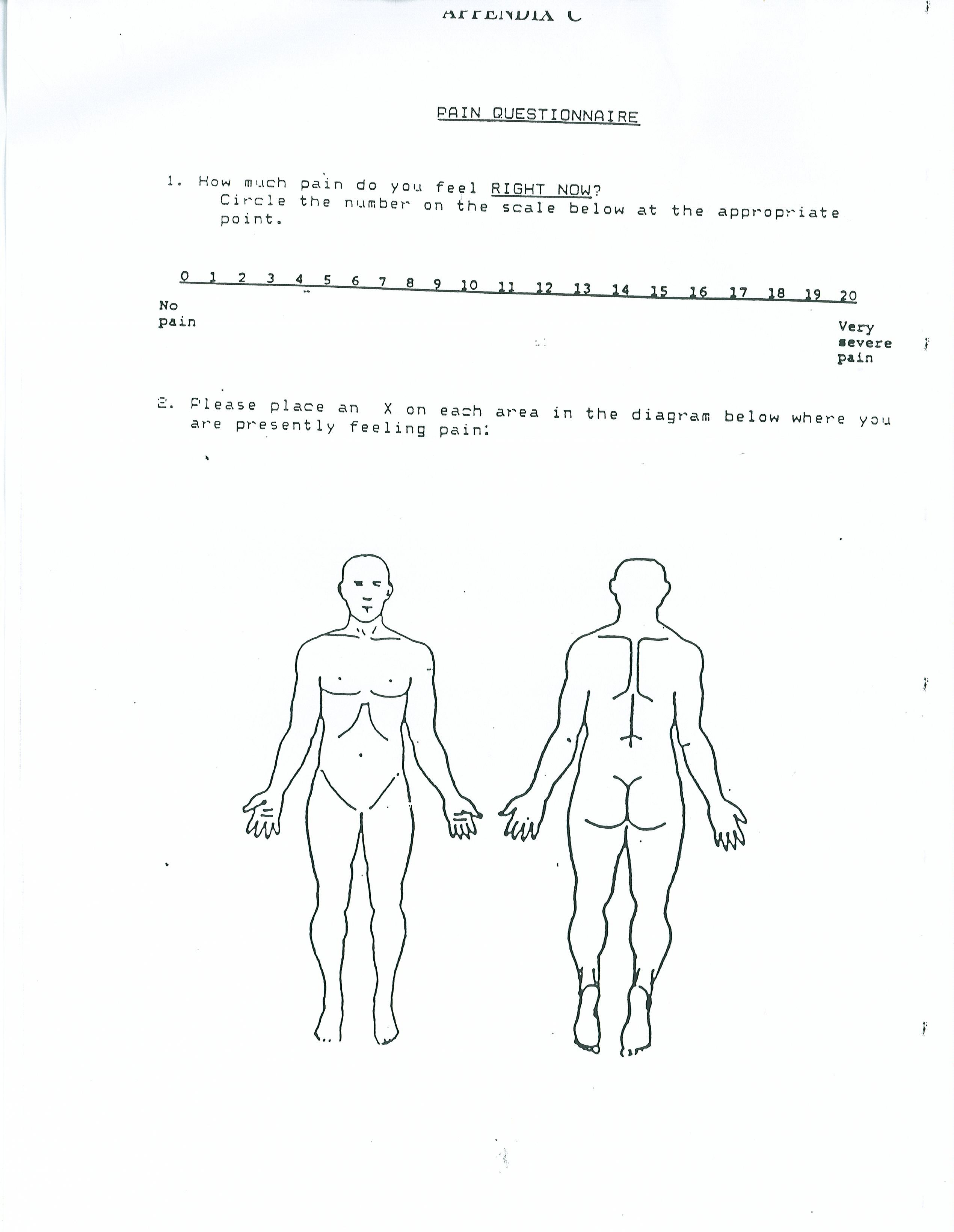
A pilot study was conducted, and modifications were made for the final study. The final research study was conducted over three months. Initially, all subjects were asked to state information regarding current health status, medications, and previous fibromyalgia treatment on a written patient demographic profile (Appendix A), adapted from the Fibromyalgia Impact Assessment. A modified Fibromyalgia Impact Assessment (FIA), pain scale, photographical postural analysis, and observational video analysis of gait served as the pre-test and post-test measurements. The modified FIA consisted of the following five sections: functional mobility, fibromyalgia pain, sleep and fatigue, work, and level of tension (Appendix B). The pain scale was numerically arranged from 0 to 20, with "0" equivalent to no pain, and "20" representing very severe pain (Appendix C). Also included with the pain scale were anterior and posterior body diagrams on which the subjects marked areas of pain.

Figure 1
A modified FIA and pain scale were completed by each subject; the former was administered verbally. For postural assessment, three full body photographs (anterior, posterior and right lateral views) of each individual standing in front of a grid were taken (Figure 1). (15) Subjects wore a bathing suit or other appropriate attire. A plumb line suspended from the ceiling was used to represent a line of reference. (27) The tripod of the camera was positioned at the same distance from the grid/subject for pre-test and post-test measurements. For the anterior and posterior views, the fixed reference point used to align the subject with the plumb line was the point midway between the heels. (27) For the right lateral view, the individual was aligned with the fixed reference point slightly anterior to the right lateral malleolus. (27) Lastly, while being videotaped in an anterior-posterior view, each subject was instructed to walk towards and away from the video camcorder twice. To ensure consistent objective measurements, investigators acted independently in gathering data; one experimenter was in charge of administering the written assessment tools, another was responsible for postural photography, and the third investigator videotaped each subject's gait.
For the duration of the study, subjects were instructed to continue taking their medications as currently prescribed. For two months, subjects met twice per week for one hour Feldenkrais ATM lessons, taught and verbally instructed by a physical therapist, certified as a Feldenkrais practitioner. The ATM lessons were sequenced specifically for individuals with chronic pain; the sixteen lessons were designed to be simplified and access normal daily postural movement strategies, such as flexion, extension, sidebending and rotation. (23,28) Subjects were positioned in prone, supine or sidelying during the lessons, and when unable to perform a particular movement secondary to pain, subjects were encouraged to visualize and imagine the movement. In addition, subjects were asked to practice that same instructed lesson on tape once daily on "non-instructional" days. In order to record *the precise number of Feldenkrais lessons performed, attendance was taken at each session, and each subject was given a monthly calendar on which to indicate whether or not a taped lesson was practiced at home.
At the conclusion of the eight weeks of classroom instruction, subjects were placed on a four week home program in which they were asked to continue practicing the taped Feldenkrais lessons, once daily at home. To encourage compliance, a check-off calendar was provided for each subject, and investigators made one follow-up phone call to each subject midway through the home program.
Following the home program, subjects reconvened to complete the post-test measurements. Subjects were allowed to see previous modified HA and pain scale scores. (29) Lastly, subjects completed a written post-study questionnaire, created to elicit feedback and any comments regarding the study (Appendix D).
Data Analysis:
A five point scale was utilized to score the modified FIA. Depending on how each question was phrased (either positively or negatively biased), the value of the answer was accommodated such that the scale of the scores was reversed for some questions. For example, if a question (i.e. Appendix B - Sect. 1, Question #4) tended to be negatively biased, "All Days" would be scored as 1 point and "No Days" scored as 5 points. Overall, a subject with a higher positive modified FIA score corresponded with a "better" overall health status.
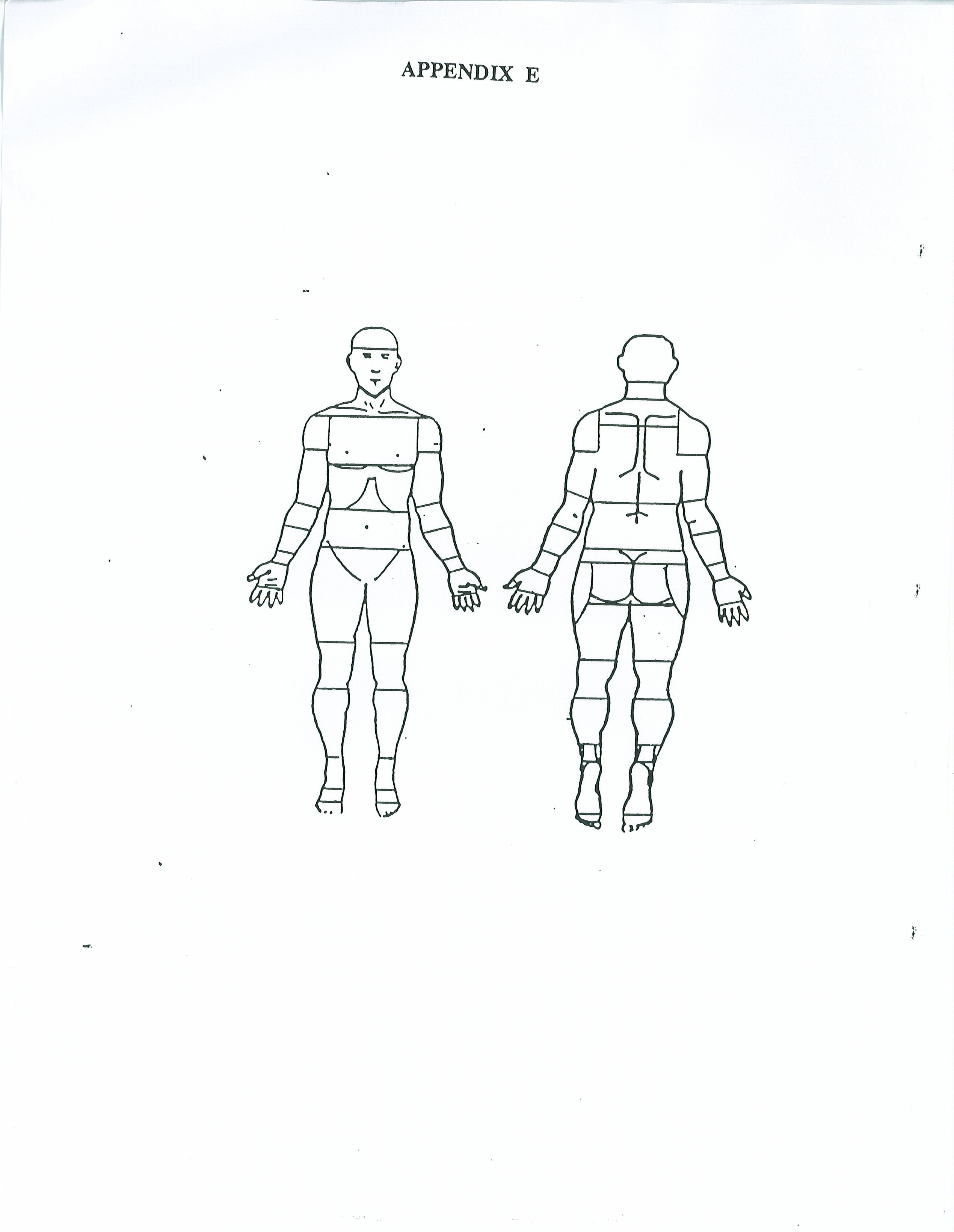
The body diagrams, which accompanied the pain scale, were logically divided into specified regions of the body (Appendix E). From these diagrams, total number of painful regions and location of pain could be identified.
The postural photographs were analyzed randomly by a physical therapist to determine the presence and severity (minimal, moderate and severe) of common postural deviations, given a form with a broad list of descriptors (Appendix F).
Lastly, the observational gait analysis for each subject was performed randomly by another physical therapist, who noted any changes in head alignment, shoulder symmetry, arm swing and pelvic symmetry.
Due to the small sample size, data was analyzed descriptively (mean, standard deviation, percentage change), with the exception of a paired t-Test, p<0.05 performed on the modified FIA and pain scale.
Results
Five subjects completed the study and were included in the final data analysis. Total compliance for these five subjects, which included attending the group lessons and practicing the tapes daily, ranged from 51.1% to 76.1% Attendance to the group lessons ranged from 68.7% to 87.5%. Compliance with practicing the taped lessons ranged from 45.8% to 73.6% (Table 2).
Table 2: Lessons and Practice Compliance
SUBJECT # | LESSONS ATTENDED (16) | DAYS PRACTICED (72) | TOTAL COMPLIANCE (88) |
1 | 14 | 53 | 67 |
2 | 11 | 38 | 49 |
3 | 11 | 34 | 45 |
4 | 14 | 33 | 47 |
5 | 14 | 49 | 63 |
( ) = maximum # lessons &/or days
Improvements were recorded in the total modified FIA scores (p<0.05) as well as in each section of the modified FIA. Significant improvement, however, was reached only for the pain and sleep/fatigue sections as well as for the total score of the modified FIA (p<0.05). (Fig. 2) A nonsignificant trend of improvement was also noted in the level of tension section (Table 3). Four out of five subjects improved their total modified FIA scores, with the greatest percentage change being 35.7% (Table 4). Three out of five subjects improved their scores in the functional mobility section, with the greatest percentage change at 25.0%. All five subjects improved their scores in the pain section, with percentage changes ranging from 30.8% to 53.8%. The sleep/fatigue section also showed improvement in all five subjects, with improvements ranging from 6.3% to 60.0% change. Three of five subjects improved in the work section, with the greatest percentage change being 25.0%. In the level of tension section, three of five subjects improved their scores, with the greatest improvement being 77.8%.
Table 3: Modified FIA mean scores (standard deviation) and p-values
SECTION # | PRE-TEST MEAN (SD) | PRE-TEST MEAN (SD) | P-VALUE |
#1 – functional mobility | 43.2 (9.149) | 45.6 (5.505) | 0.381 |
#2 – fibromyalgia pain | 12.2 (3.633) | 17.0 (4.950) | 0.003* |
#3 – sleep/fatigue | 13.4 (4.775) | 17.6 (5.505) | 0.022* |
#4 – work | 12.4 (4.278) | 13.2 (3.421) | 0.242 |
#5 – level of tension | 13.2 (2.588) | 17.0 (3.3536) | 0.106 |
Total Scores | 94.4 (20.403) | 110.4 (18.515) | 0.046* |
* significant at p < 0.05
 Figure 2
Figure 2
Table 4: Individual modified FIA scores with percentage change
SECT # | SUBJECT #1 | SUBJECT #2 | SUBJECT #3 | ||||||
PRE | POST | % | PRE | POST | % | PRE | POST | % | |
#1 (60) | 53 | 52 | -1.9 | 44 | 48 | 9.1 | 32 | 37 | 15.6 |
#2 (30) | 17 | 23 | 35.3 | 7 | 10 | 42.9 | 11 | 15 | 36.4 |
#3 (35) | 20 | 25 | 25.0 | 8 | 10 | 25.0 | 10 | 16 | 60.0 |
#4 (20) | 17 | 18 | 5.9 | 16 | 15 | -6.3 | 8 | 10 | 25.0 |
#5 (30) | 14 | 22 | 57.1 | 13 | 13 | 0 | 9 | 16 | 77.8 |
Total (175) | 121 | 140 | 15.7 | 88 | 96 | 9.1 | 70 | 94 | 34.3 |
SECT # | SUBJECT #4 | SUBJECT #5 | ||||
PRE | POST | % | PRE | POST | % | |
#1 (60) | 36 | 45 | 25.0 | 51 | 46 | -9.8 |
#2 (30) | 13 | 20 | 53.8 | 13 | 17 | 30.8 |
#3 (35) | 13 | 20 | 53.8 | 16 | 17 | 6.3 |
#4 (20) | 8 | 10 | 25.0 | 13 | 13 | 0 |
#5 (30) | 14 | 19 | 35.7 | 16 | 15 | -6.3 |
Total (175) | 84 | 114 | 35.7 | 109 | 108 | -0.9 |
( ) = maximum score possible, % = percentage change pre. vs post.
Mod FIA sections: #1 = functional mobility; #2 = fibromyalgia pain;
#3 = sleep/fatigue; #4 = work; #5 = level of tension
 Figure 3
Figure 3
The paired t-Test performed on the pain scale did not prove to be significant at the 95% confidence interval (p<0.05), with a p-value of 0.486. (Fig. 3) Two subjects reported decreased pain scores, while two subjects reported slightly increased pain scores. One subject reported the same pain score. Four subjects reported a decrease in the number of areas of pain on the body diagram, while one subject reported an increase in the number of pain spots (Table 5, Fig. 4).
Table 5: Pain scores
SUBJECT # | PAIN SCALE (0-20) | # PAIN REGIONS | ||
| PRE | POST | PRE | POST |
1 | 7 | 2 | 10 | 7 |
2 | 14 | 11 | 33 | 44 |
3 | 13 | 15 | 20 | 18 |
4 | 14 | 14 | 20 | 12 |
5 | 9 | 10 | 13 | 8 |
Minimal improvements in posture were noted, with the majority of these being in the alignment of the head and feet. Four of the five subjects demonstrated more neutrally aligned feet while three of the five subjects demonstrated the head to be more neutrally aligned on the neck. There were areas of the body observed to be less neutrally aligned for all five subjects.
Minimal improvements were also noted in gait. Three of the five subjects had improved arm swing. One subject was observed to have a more symmetrical pelvis during gait. Some negative changes were noted in the head alignment of two subjects and in the shoulder symmetry and arm swing of another subject.
In the post-study feedback questionnaire, four subjects reported that the Feldenkrais method helped them become more aware of their body, its movement patterns and limitations. Two subjects stated that the Feldenkrais method did not seem to help their pain, two subjects did not address pain on the feedback questionnaire, and only one subject reported that the Feldenkrais method helped to decrease her pain.
Although Subject 6 was excluded from the group data analysis secondary to an acute onset of a medical condition, it is interesting to report her individual results, since she did complete the study. Her total compliance was 33%, with a lesson attendance of 81% and daily tape practice of 22%. She improved her total modified FIA score from 75/175 pre-test to 90/175 post-test, with improvements in each individual section except for section 1 (functional mobility), in which her score decreased slightly. Her pain scale score decreased from 10 to 7 on the 20 point scale and the number of spots, in which she reported pain on the body diagrams, decreased from 13 to 5. In reference to the postural analysis, the subject's knees, shoulders and clavicles were noted be more neutrally aligned. The subject's head, lumbar spine and feet were found to be slightly less neutrally aligned. No significant changes were noted in gait analysis, except subject's head was slightly aligned to the right. On the post-study feedback questionnaire, she noted that the Feldenkrais method brought awareness to areas of her body that were painful, and helped her learn to change body movement patterns to help decrease the pain.
Discussion
Pain, sleep/fatigue sections and overall total of the modified FIA were found to be statistically significant in our sample of subjects as a whole. This suggests that the Feldenkrais method has potential value in reducing pain and decreasing fatigue in fibromyalgia patients, as measured by the modified FIA. However, it is interesting to note that the pain scale scores, as a group, did not show significant improvement. Three subjects reported the same or worse pain on the pain scale but reported improved scores on the pain section of the modified FIA. One possible reason for this would be that the modified FIA pain section asks the subject to report to whaf degree pain interferes with their daily activities and sleep, in addition to asking the subject how often they experienced pain and its severity. The 20 point pain scale simply asks the subject to report the intensity of the pain at that specific point in time. Perhaps the subjects had severe pain less often over the four week period or perhaps other changes (i.e. decreased level of tension and fatigue, or increased body awareness) made it possible to perform their daily activities, therefore improving their modified FIA pain score. This hypothesis is supported by the statistical significance of the sleep/fatigue section of the modified FIA, and the fact that four of five subjects reported that the Feldenkrais method improved their body awareness on the post study feedback questionnaire. As a whole, our results support this hypothesis. Fibromyalgia patients are prone to unpredictable flare-ups during the course of their condition, which may have caused their pain scale scores to increase or decrease at a specific point in time. (30) The statistical significance of the total modified FIA scores suggests a possible improvement in the overall health status of the subjects in our study, although subject S reported no significant change. The functional mobility, work and level of tension sections of the modified FIA did not prove to be statistically significant. Our small sample size could possibly explain this for the level of tension section (p=0.11). A longer duration with the lessons and/or practice tapes may be required to see changes in these sections. Nelson states in regards to the Feldenkrais method, "A reasonable amount of time must be allotted to absorb what is learned...Students are encouraged to learn at their own pace." (23) It is also possible that the patients did not fully understand the concepts behind the Feldenkrais method. The subjects may not have had a kinesthetic sense that was sensitive enough to apply the verbally instructed movement concepts of the method. Understanding the concepts of the Feldenkrais method and its premises is important for each subject, as they need to be able to relearn comfortable movement patterns, reorganizing them at the central nervous system level. (23,24) Perhaps inclusion of FI, the hands-on, individualized form of the Feldenkrais method, would have been beneficial to enhance each subject's kinesthetic sense and awareness, enabling them to more fully understand the premises and concepts of the method. The ATM group lessons were analyzed specifically to see if this would provide a more cost effective form of the method in light of today's changing health care. However, further analysis of FI is warranted.
It is interesting to note that three of the five subjects reported fairly significant positive percentage changes on the level of tension section of the modified FIA. It is also important to remember that other variables, such as personality, background, learning style, or stressful events occurring during the course of the study may have affected the results in all sections of the modified FIA.
As mentioned earlier, when looking at the post-study feedback questionnaire, we found that four out of five subjects stated that they felt the Feldenkrais method made them more aware of their body and its movements. According to the literature, one of the primary claims of the Feldenkrais method is that it functions to increase awareness of physical movement by improving kinesthetic sense. (18) Subject feedback from this study supports this claim. This enhanced body awareness may be a reason for the significant improvement in the pain section for all five subjects and improvement in the level of tension section for three of the five subjects. The subjects may have felt more confident in their ability to make movement choices, thereby decreasing anxiety and stress in daily activities. If it is possible to decrease pain through use of the Feldenkrais method, as measured by the 20 point pain scale,-it may be necessary for a person to first improve their kinesthetic sense, increasing their movement choices, and then learn to make the most comfortable choices.
The Feldenkrais method also incorporates mental imagery as a means to enhance body awareness, primarily in situations when a person has difficulty performing the movements. Fairweather and Sidaway found that ideokinetic imagery training produced positive postural alignment changes in high school and college students with and without low back pain, especially when combined with kinesthetic awareness activities. (22) Warner and McNeill conducted a review of literature regarding the effects of mental imagery and practice on physical skills and found that mental imagery and practice have been consistently shown to produce physical results and enhance motor learning in the areas of sports and health care services when training is conducted over time. (21) One's ability or willingness to imagine movement, the sensitivity of one's kinesthetic sense and the amount of time allotted for training are factors that may have come into play or interacted in our study to impact the effectiveness of the Feldenkrais method on each individual subject.
A final factor which may have influenced the results of our study were the compliance rates, since the Feldenkrais method claims to be more effective when used consistently over time as would any motor learning method. Some possible reasons for missed lessons and practice days would include the daily drive to the site of the study. Several subjects informally expressed a concern that this may have contributed to their level of stress and fatigue. The fluctuating nature of fibromyalgia symptoms may have also made it difficult for subjects to be consistent. There were also occasional scheduling conflicts for each of the subjects that could not be helped. Overall, however, compliance rates in our study were fairly high, ranging from 51.1% to 76.1%, including attending group sessions and practicing lessons daily at home. Compliance to attending group lessons was higher than compliance with practicing daily lessons.
Subject 6, who was excluded from data analysis but completed the study, was an interesting case to analyze. Although her compliance was fairly low, probably due to her acute medical conditions, she showed improvement in her total modified FIA scores, as well as in each separate section with the exception of the functional mobility section. She also reported a decreased pain scale score. Subject 6 has a background in dance and has been involved in other therapy that emphasizes development of kinesthetic awareness. This would suggest that a person with a particular background, perhaps one that involves other kinesthetic awareness training, may respond more positively and/or more quickly to the Feldenkrais method. Subject 6 also reported on her post-study feedback questionnaire that she felt an enhanced body awareness, and stated several specific areas of her body where she observed improvement.
Future studies in the area of fibromyalgia and the Feldenkrais method may include ones that measure the reliability and/or validity of the modified FIA, since it is different in organization, scoring and content than the original FIA. It might also be helpful to quantify gait changes by analyzing velocity, stride length, step length, cadence, and other parameters (i.e. functional activities). A study with a longer time frame of lessons and/or practice days would be helpful to look at the long term effects of the Feldenkrais method on fibromyalgia patients. It would also be interesting to look at a study beginning with individualized, hands-on Functional Integration, then moving subjects into a program of group ATM lessons. This might increase understanding of the concepts of the Feldenkrais method, as well as satisfy the move towards more cost-effective health care. After data collection was completed, FI was performed on one individual who reported increased understanding of the concepts of the method. Also, a larger sample size with a control group receiving traditional physical therapy would perhaps shed more light on the effects of the Feldenkrais method and its potential use as an adjunct to the physical therapy treatment of selected fibromyalgia patients. Lastly, due to the discrepancy between pain scale scores and FIA pain section results, the perception of pain continues to warrant further investigation.
Summary
In conclusion, the Feldenkrais method has potential value as a possible adjunct to the physical therapy treatment of selected fibromyalgia patients, as evidenced by the statistical significance of the pain and sleep/fatigue sections and the total modified FIA scores. The key points are:
- Those who improve their kinesthetic sense and mental imagery may have more success with the method.
- Increased body awareness, reported by four out of five subjects, may be a bridge to more comfortable, efficient movement, which may decrease pain and fatigue over time.
- If able to move more comfortably, fibromyalgia patients might increase participation in aerobic exercise and other treatments.
- ATM lessons are a cost-effective way to increase body awareness.
Acknowledgements
Mark Reese, PhD, CFP
The Reese Movement Institute, Inc., Cardiff by the Sea, CA
Lawrence W. Goldfarb, PhD, CFP
Champagne, Illinois
MSMC Physical Therapy Department
Los Angeles, CA
Monique Peterson, PT, OCS
Robyn Smith Physical Therapy, Manhattan Beach, CA
Craig Newsam, MPT
Ranchos Los Amigos Medical Center, Downey, CA
Marilyn Pink, MS, PT
Centinela Biomechanics Lab, Los Angeles, CA
South Bay Hospital - Physical Therapy Department
Torrance, CA
The Center for Physical Health
Los Angeles, CA
Dorothy Johnson, RN
Southern California Arthritis Foundation
Southern California Fibromyalgia Support Groups
Ken Nies, MD & Richard Goldin, MD
Torrance, CA
Peng Fan, MD & Associates
Van Nuys, CA
Gideon Darvish, MD
Inglewood, CA
Cinder Marshall, MD & Associates
Inglewood, CA
BIBLIOGRAPHY
- Nies KM. Treatment of the fibromyalgia syndrome. The Journal of Musculoskeletal Medicine. 1992 May, 9(5): 20-6.
- Guler M, Kirnap M, Bekaroglu M, Uremek G, Onder C. Clinical characteristics of patients with fibromyalgia. Israel Journal of Medical Sciences. 1992 January, 28(1): 20-3.
- Reilly PA, Littlejohn GO. Current thinking on fibromyalgia syndrome. Australian Family Physician. 1990 October, 19(10): 1505-8, 1511-2, 1516.
- Waylonis GW, Heck W. Fibromyalgia syndrome: new associations. American Journal of Physical Medicine and Rehabilitation. 1992 December, 71(6): 343-8.
- Turner M. Posture and pain. Physical Therapy Review. 1957, 37(5): 294-7.
- Griegel-Morris P, Larson K, Mueller-Klaus K, Oatis CA. Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Physical Therapy. 1992 June, 72(6): 425-30.
- Scudds RA, McCain GA, Rollman GB, Harth M. Improvements in pain responsiveness in patients with fibrositis after successful treatment with amitriptyline. Journal f Rheumatology. 1989 November, Supplement, 19: 98-103.
- Bennett RM. Beyond fibromyalgia: ideas on etiology and treatment. Journal of Rheumatology. 1989 November, Supplement, 19: 185-91.
- Goldman JA. Hypermobility and deconditioning: important links to fibromyalgia/fibrositis. Southern Medical Journal. 1991 October, 84(10): 1192-6.
- Kiug GA, McAuley E, Clark S. Factors influencing the development and maintenance of aerobic fitness: lessons applicable to the fibrositis syndrome. Journal of Rheumatology. 1989 November, Supplement, 19: 30-9.
- McCain GA, Bell DA, Mai FM, Halliday PD. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis and Rheumatism. 1988 September, 31(9): 1135-41.
- McCain GA. Role of physical fitness training in the fibrositis/ fibromyalgia syndrome. The American Journal of Medicine. 1986 September 29, 81(Supplement 3A): 73-7.
- Bennett RM, Clark SR, Goldberg L, Nelson D, Bonafede RP, Porter J, Specht D. Aerobic fitness in patients with fibrositis: A controlled study of respiratory gas exchange and xenon clearance from exercising muscle. Arthritis and Rheumatism. 1989 April, 32(4): 454-60.
- Nichols DS, Glenn TM. Effects of aerobic exercise on pain perception, affect, and level of disability in individuals with fibromyalgia. Physical Therapy. 1994 April, 74(4): 327-332.
- Lake B. Acute-back pain: treatment by the application of Feldenkrais principles. Australian Family Physician. 1985 November, 14(11): 1175-8.
- Wanning T. Massage, acupuncture, yoga, t'ai chi, and Feldenkrais. American Association of Occupational Health Nurses Journal. 1993 July, 41(7): 349-51.
- Narula M. Effect of the six-week Awareness Through Movement lessons - the Feldenkrais Method on selected functional movement parameters in individuals with rheumatoid arthritis. Masters' Thesis from Oakland University in Rochester, Michigan. 1993, pp. 1-122.
- Peterson R. Feldenkrais integrates body and brain through movement. Wholistic Living News. 1988 February.
- Zemach-Bersin D. Zemach Bersin K, Reese M. Relaxercise: The Easy Way to Health and Fitness. 1990, Harper & Row, Publishers, Inc., San Francisco.
- Brown E, Kegerreis S. Electromyographic activity of trunk musculature during a Feldenkrais Awareness Through Movement Lesson. Isokinetics and Exercise Science. 1991, 1(4): 216-21.
- Warner L, McNeill ME. Mental imagery and its potential for physical therapy. Physical Therapy, 1988 April, 68(4): 516-21.
- Fairweather MM, Sidaway B. Ideokinetic imagery as a postural development technique. • • h •uart-rl for Exercise and Sport. 1993 December, 64(4): 385-92.
- Nelson SH. Playing with entire self: the Feldenkrais method and musicians. Seminars in Neurology. 1989 June, 9(2): 97-104.
- Wildman F. Learning - the missing link in physical therapy. Physical Therapy Forum. 1988 February, 7(6): 1,3-5.
- Goldfield EC. Dynamic systems in development: action systems. A Dynamic Systems Approach to the Development of Cognition and Action, editors: Thelen E & Smith LB. 1994, Cambridge, MA: MIT Press, pp. 51-70.
- Ruth S, Kegerreis S. Facilitating cervical flexion using a Feldenkrais method: awareness through movement. JOSPT. 1992 July, 16(1): 25-9.
- Kendall, FP. Muscles: Testing and Function - Fourth Edition with Posture and Pain. 1993, Williams & Wilkins, Baltimore, Maryland. pg. 71 - 72, 100.
- Mark Reese, PhD, CFP. The Reese Movement Institute, Inc., Cardiff by the Sea, California.
- Guyatt GH, Be°rman LB, Townsend M, Taylor DW. Should Study Subjects See Their Previous Responses? I Chron Dis. 1985, 38 (12): 1003-1007.
- Fan PT, Blanton ME. Clinical features and diagnosis of fibromyalgia. The Journal of Musculoskeletal Medicine. 1992 April, 9(4): 24-4
- Ruth S, Kegerreis S. Facilitating cervical flexion using a Feldenkrais method: awareness through movement. JOSPT. 1992 July, 16(1): 25-9.
- Kendall, FP. Muscles: Testing and Function - Fourth Edition with Posture and Pain. 1993, Williams & Wilkins, Baltimore, Maryland. pg. 71 - 72, 100.
- Mark Reese, PhD, CFP. The Reese Movement Institute, Inc., Cardiff by the Sea, California.
- Guyatt GH, Be°rman LB, Townsend M, Taylor DW. Should Study Subjects See Their Previous Responses? I Chron Dis. 1985, 38 (12): 1003-1007.
- Fan PT, Blanton ME. Clinical features and diagnosis of fibromyalgia. The Journal of Musculoskeletal Medicine. 1992 April, 9(4): 24-4
(2008). Awareness Through Movement Sequence on Fibromyalgia Patients.
Feldenkrais Research Journal. 4,
| Attachment | Size |
|---|---|
| APPENDIX A.pdf | 100.74 KB |
| APPENDIX B.pdf | 116.03 KB |
| Appendix C.jpg | 262.64 KB |
| APPENDIX D.pdf | 4.59 KB |
| Appendix E-image.jpg | 225.57 KB |
| APPENDIX E.pdf | 98.53 KB |
| APPENDIX F.pdf | 118.36 KB |
{kind=link}
{kind=link}